As the overdose prevention program director for Project Weber/RENEW— an addiction recovery organization in Providence— Dennis Bailer is a professional when it comes to teaching people how to save lives. But even years of training and leading demonstrations couldn’t have prepared him for the gut wrenching feeling that would hit when he witnessed someone overdosing for the first time in 2018.
“It was nerve-wracking,” he admitted, “but I just followed the same steps that I’ve been telling other people to do for years.”
On the day of the overdose, Bailer had the good fortune of being at work in his office, then located on Allens Avenue in Providence. That afternoon, a young couple came into the office’s drop-in community center, obviously high on opioids.
“I clearly recognized the signs,” Bailer said in an interview, “the nodding [of the head] and the lethargy. The gentleman stayed in the drop-in center but the woman got up and went to the restroom.”
Five minutes went by with no sign of the woman, and Bailer began to worry. A heavy pounding on the bathroom door produced no response.
“I cracked the door open to look for her,” he said, “and she was out on the floor with a needle beside her.”
Almost immediately, Bailer noticed the icy blue ring around the woman’s lips, a telltale sign of deoxygenation. Individuals suffering an opioid overdose need to receive help within a matter of minutes, otherwise lack of oxygen flowing throughout the body will kill both their heart and brain. There is only one tool that can reverse these effects, and its presence or absence is quite literally a matter of life or death: “Narcan. I knew right away that I needed to get Narcan.”
After dialing 911, Bailer administered a kit (equal to one dose) of Narcan, the brand name of the now-famous opioid antagonist naloxone, but nothing happened. Then he delivered a second dose. It still wasn’t working and there was no Emergency Medical Service (EMS) personnel in sight. The woman only regained consciousness after three doses of the drug, all of which Bailer administered in the roughly six minutes before EMS arrived to bring her to the hospital.
Without naloxone, the woman would have joined the list of over 300 people in Rhode Island who died of an opioid overdose in 2018.
Bailer’s story underscores the lifesaving impact this drug can have— if it gets into the right hands.
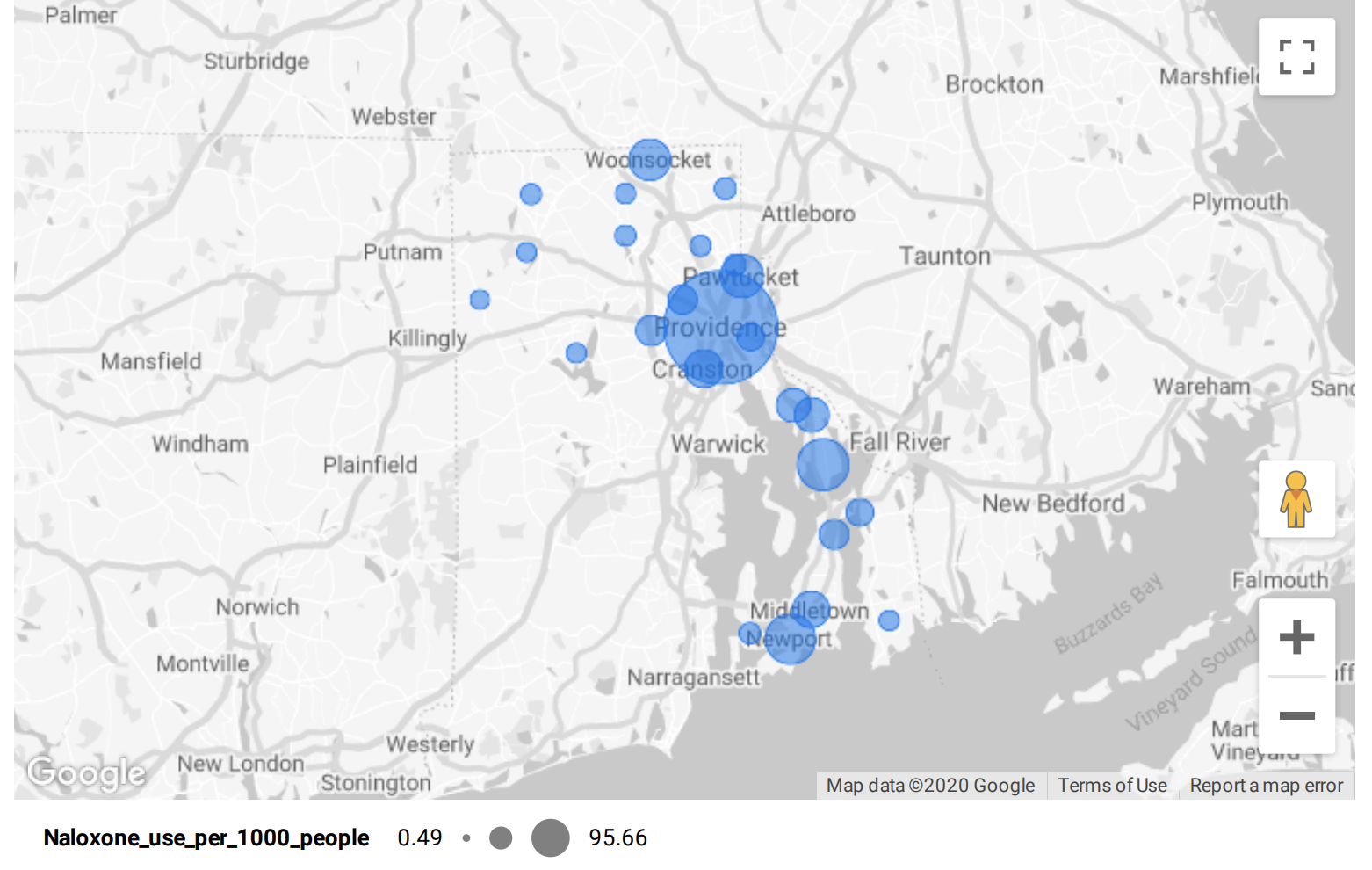
Since 2016, naloxone has been administered over 10,000 times in Rhode Island according to data from the Rhode Island Department of Health (RIDOH), with the number of uses increasing steadily each year. In 2019, the drug was used 2,667 times across the state, with the majority of applications coming from the major cities: Cranston, Pawtucket, Providence, Warwick, and Woonsocket. These five municipalities alone accounted for nearly 70% of naloxone uses last year (69.1%) and are also responsible for some of the biggest leaps in usage over time.
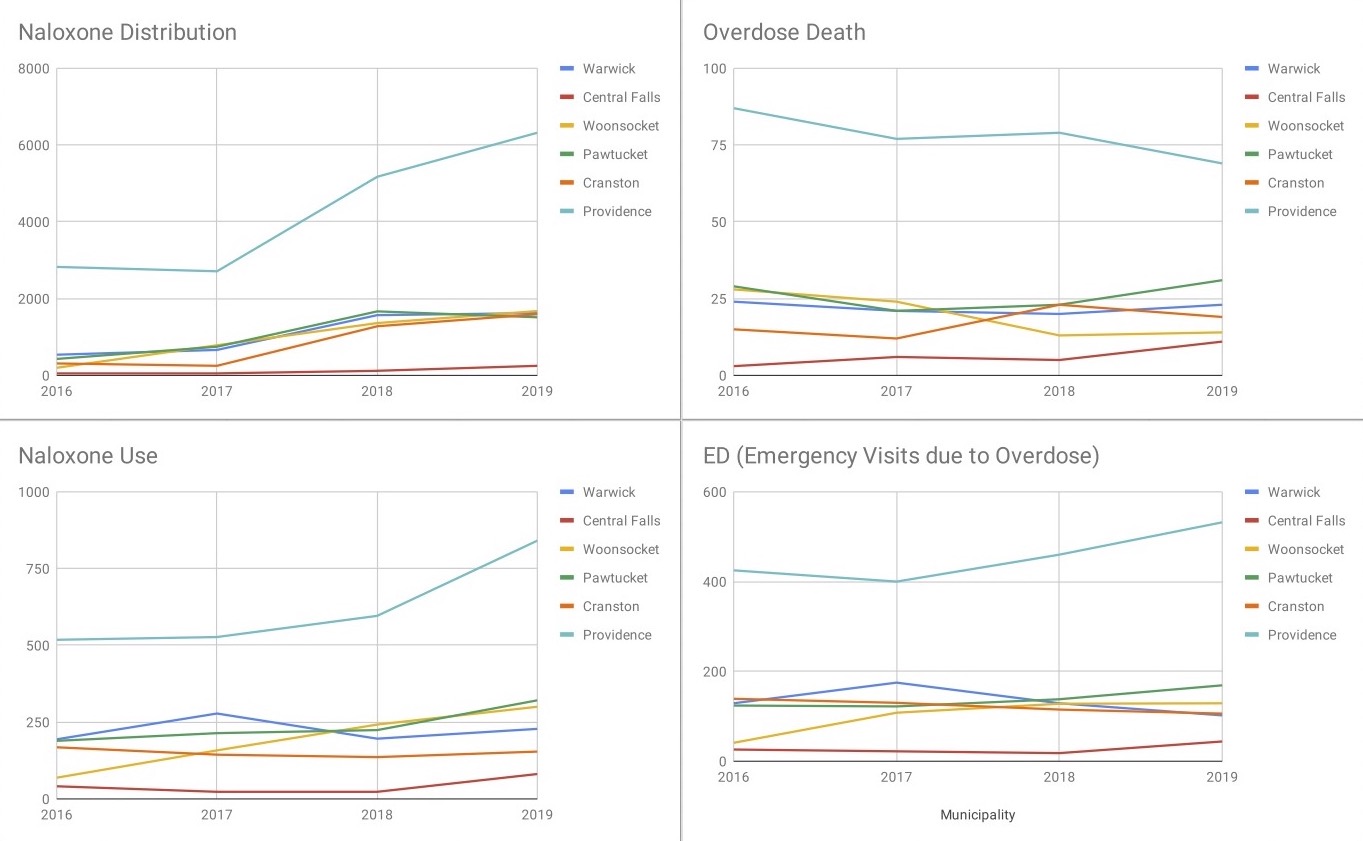
Many Rhode Island cities and towns both large and small have seen their naloxone usage remain the same or decrease in the past four years, almost always in proportion to a decrease in the number of overdoses overall. But data from several municipalities reflects that the number of people overdosing on opioids has remained relatively constant, or even increased, over time. What is different is that — up until March 2020, when opioid fatalities spiked during the pandemic — fewer people have been dying from their overdoses, likely because of Narcan.
Take Providence, for example, where the number of overdose fatalities decreased from 87 in 2016 to 79 in 2018, and then again to 69 deaths in 2019. During this time, opioid-related emergency department visits shot up from 425 to 460, and then up to 532. As for naloxone usage, it increased 62.5% between 2016 and 2019, suggesting that increased application is in fact saving lives. These trends also appear in municipal data from North Kingstown and Woonsocket, where the number of fatal opioid overdoses has been cut in half since 2016, while both hospital emergency department visits and naloxone use more than tripled.
For the dozens of members on the Prevent Overdose RI Taskforce, these numbers both inspire hope and serve as a reminder that there is a lot more work to be done. Only three municipalities in the State of Rhode Island survived 2019 without any opioid overdose deaths— and of those three, only the Town of Little Compton made it through the year without any reported overdoses at all.
Referred to in many pharmacies as “the opioid antidote,” naloxone has played a crucial role in saving the lives of Rhode Islanders experiencing an overdose. In many cases, it’s the only thing that can.
Its efficacy remains limited to the number of people who carry it with them and know how to use it, but fortunately, that number is growing. Narcan and other naloxone products are beginning to be placed inside high schools, churches, and more recently, courthouses. Superior Court Justice Kristin E. Rodgers, who works regularly with the task force, was one of the judges who pushed to have naloxone installed inside the Licht Judicial Complex in Providence, and she’s glad she did.
“We have Narcan here now, and already we’ve had to use it once or twice,” she said. “With the Governor’s task force, we’re trying to get it in more places because it really is life-saving.”
Meanwhile at schools across the state, a law passed in 2015 took what one publication called the country’s “most aggressive approach” to overdose prevention and mandated that naloxone be stocked in all public middle and high schools. Nurses from various high schools in the Providence, Woonsocket, and Central Falls School Departments all confirmed that they’ve never had to use it, but each of their offices has a kit or two, just in case.
Nevertheless, every year there are some users who slip through the cracks, and everyone from firefighters to pharmacists are trying to figure out who they could be missing—and why.
“I’m not sure where they are, but we’re missing some of the population,” said Collette Onyejekwe, a former pharmacist who now works for RIDOH, educating medical personnel on best practices for prescribing drugs to patients. Onyejekwe said that she could recall “two instances where individuals came into the community pharmacy I was working at to get naloxone, but their friend already overdosed.”
Although it is widely known among the medical community that naloxone needs to enter the system within a matter of minutes in order to reverse the effects of an overdose, “these individuals left their friend unattended [and] drove fifteen minutes to the pharmacy to pick up the naloxone.” Little did these people know that their efforts were too little, and far too late.
Both Bailer and Onyejekwe stressed the importance of dialing 911 as the first step after witnessing any overdose, but Onyejekwe explained that for many people unfamiliar with the laws surrounding overdoses, the thought of calling for help can seem even more dangerous than trying to solve the problem alone.
“One individual [who came into the pharmacy] was trying to avoid prosecution. She didn't know anything about our Good Samaritan laws,” said Onyejekwe, adding that the young woman’s thoughts were decidedly “more concerned with ‘I'm going to face prosecution,’ than ‘I need to contact 911.’”
The law Onyejekwe is referring to is one of two bills passed by the Rhode Island General Assembly during the summer of 2018 to increase naloxone access and availability. The first required the RIDOH to develop and distribute guidelines for “co-prescribing” naloxone when also prescribing an opioid to patients who are at an elevated risk of overdosing, while ensuring health insurance reimbursement. The second bill amended Rhode Island’s Good Samaritan law, which already protected people from arrest for helping an individual suspected of overdosing. The amendment allowed police and medical personnel to hand out naloxone kits to individuals considered to be at risk for overdose, as well as to their friends and family.
Data from before and after this legislation reflects that while the distribution of naloxone has soared, shooting up over 330% in just three years, its usage has increased much more gradually. One major reason for the slower rise in usage, Onyejekwe pointed out, is the price tag.
Although RIDOH advertises that all health insurers in Rhode Island cover at least one type of generic naloxone with a no-cost or low-cost co-payment, that development is fairly new and not always widely-known. Onyejekwe recalled several occasions over the past two years when patients would arrive at the pharmacy with two prescriptions from their physician: one for a pain medication with a $3 copay, the other for Narcan, with a $50 copay.
“People are always like, ‘I'm not paying for that. The doctor said I don't need it, it’s only just in case. I don't have the money, I’m not picking that up,’” she said.
Until recently, the lowest out-of-pocket price for patients hoping to buy Narcan without insurance was $94.99. Although the FDA approved the country’s first generic naloxone hydrochloride nasal spray in April 2019, which can be purchased at the pharmacy for as little as $30, that’s still ten times the price of the copay for the opioid itself. And $30 is still way outside of the price range for many low-income patients, meaning that dozens of people a year begin taking incredibly powerful prescription opioids without ever gaining access to naloxone, or learning how to use it.
Equally concerning, many doctors are still familiarizing themselves with naloxone co-prescribing laws, often relying on pharmacists like Onyejekwe to remind them when they forget to write their patients a dual prescription.
“I love that we had the Naloxone campaign last year,” said Onyejekwe, “because even when I was going out to drop off signs at the pharmacies, I met one pharmacist who had been practicing for many years who said, ‘I have an honest question that I want to ask you. Will I be prosecuted if I contact 911 or administer Narcan?’ That goes to show you that most people, including healthcare professionals, don't know the laws completely.”
As information about naloxone is increasing, so, too, is usage in different sectors of the community. For years, naloxone usage nationwide remained largely limited to emergency medical personnel, and Rhode Island was no different.
In 2012, for example, only 94 kits of naloxone were distributed across the entire state, according to the RIDOH. Even in 2015, when Rhode Island was among the top five states with the highest rates of opioid-related emergency department visits, hospitals, pharmacies, and community organizations in the state distributed fewer than 1,000 naloxone kits total.
In April 2018, however, U.S. Surgeon General Jerome Adams issued a public health advisory specifically focused on naloxone, urging more Americans to carry and learn to use the overdose-reversing drug. “It is time to make sure more people have access to this life saving medication,” said Dr. Adams, “because 77 percent of opioid overdose deaths occur outside of a medical setting.”
Shortly thereafter, Governor Gina Raimondo signed the naloxone co-prescription bill and the Good Samaritan amendment into law. As a result of these initiatives, the number of naloxone kits distributed across the state more than doubled, from roughly 7,600 in 2017 to over 17,200 in 2018. In 2019, the number of kits distributed reached 21,205: nearly triple the number from 2017 and over 225 times the 94 naloxone kits from 2012.
Many different agencies and departments are continually purchasing naloxone as needed. Linda Reilly of the state’s Department of Behavioral Healthcare, Developmental Disabilities & Hospitals said there is “no central clearinghouse that keeps all the receipts of how much Naloxone is secured within the state.”
But within her own department, Reilly confirmed that the BHDDH distributed 1,788 kits throughout the state in the first 11 months of 2020. Despite the pandemic, that’s nearly the same number of kits the agency distributed in 2019. The BHDDH distributes naloxone to various shelters and recovery centers in the state including Anchor Recovery as well as state colleges and universities including the Community College of Rhode Island, the University of Rhode Island and Rhode Island College. “We use funds from federal grants and a small amount of money from the Rhode Island Opioid Stewardship Fund, [which] is financed by manufacturers and distributors of opioids to support opioid treatment.” No taxpayer money is used to purchase the naloxone, she said.
The variety of places where naloxone is available has also increased over the past three years. Last year, community organizations like churches and recovery centers handed out 8,956 naloxone kits, nearly double the 4,553 distributed in 2017. For pharmacies, this number was over 11,000— a roughly 500% increase from 2017.
Hospitals last year gave out more than twice the number of naloxone kits than the year before, but they are the last line of defense, the places where people who have overdosed are taken for treatment. Though medical personnel administer naloxone regularly in the emergency room, they distribute fewer kits overall in Rhode Island than police, firefighters, EMT workers and community organizations do.
“Before the pandemic, it was almost every shift that I would have patients come in after an opioid overdose needing to receive naloxone,” said Dr. Rachel Wightman, an emergency room doctor at Miriam Hospital and Assistant Professor of Emergency Medicine at Brown University’s Alpert School of Medicine.
“We distribute naloxone in an opt-out fashion,” said Wightman of Miriam’s discharge procedure. “So we give naloxone to all patients with an opioid overdose and patients would have to opt out and explicitly say no to not get naloxone” when they leave the hospital.
In 2019, Miriam Hospital distributed 59 naloxone kits, the second highest number of any hospital in the state. However, there is no law or policy mandating that hospitals offer naloxone to overdose patients, and though professionals like Dr. Wightman encourage it, many patients refuse to take Narcan home with them upon discharge, insisting that another overdose “won’t happen again.”
“In my experience, right after an overdose isn’t a good time to target somebody because generally they have a lot of emotions running through their system and they’re not [emotions] of looking for help,” said Zachariah Kenyon, Deputy Assistant Chief of EMS at the Providence Fire Department, adding that many people are convinced “that they don’t have an issue and just want to go home.”
Data compiled by the Prevent Overdose RI Coalition shows that naloxone is now available at 131 pharmacies in the state and 14 community organizations. Of these community organizations, most are recovery centers and fire stations, and all provide the drug at no cost following a free overdose prevention training. Fire stations in larger municipalities like Providence have also introduced “leave-behind kits,” or packages that EMS can leave behind with the friends or family of an overdose victim that contain naloxone and a list of recovery resources.
While the distribution location has no impact on the type or quality of naloxone an individual receives, one concern raised by recovery specialists is that in-person training is generally only available when the drug is acquired at community organizations. Applying Narcan nasal spray is fairly straightforward, but nevertheless some professionals worry that civilians don’t have enough experience recognizing the signs of an overdose and administering naloxone doses via an intravenous or intramuscular applicator.
Kevin Farley, an EMT based in Portsmouth, said that the number of naloxone doses EMTs must give to reverse the effects of an overdose has skyrocketed since fentanyl was introduced into the drug market in Rhode Island around 2013.
“When I started, it used to be that the standard dose of Narcan was 2 mg and that would usually pull somebody out,” Farley said in a recent interview. “Now there are cases where we’ve given up to 10 mg and it’s barely budged ‘em.” Farley explained that laypeople who administer naloxone should focus on restoring breathing on an overdose victim, as opposed to waking them up.
Farley’s advice will likely prove quite useful given that between 2016 and 2019, the total number of patients who received naloxone from someone other than a medical professional or EMS worker has more than doubled. And research published in March 2019 in the Rhode Island Medical Journal reported that the percentage of opioid overdoses occurring in public places increased by 25% between 2016 and 2019.
Bailer of Project Weber/RENEW noted that, “the statewide statistic is that roughly one third of overdoses happen in public places. In Providence, it’s over 60%.”
For years, police were reluctant to carry naloxone with them, but according to Jason Rhodes, Chief of the Center for Emergency Medical Services at the RIDOH, “all the police departments in the state now carry Naloxone on their belt, at least a couple of doses.”
While police officers are reaching an increasing number of overdose victims, most overdose prevention workers agree that an even more widespread distribution of naloxone will be necessary to catch those people currently falling through the cracks.
According to Kenyon and data kept by the state Department of Health, the target group for overdose prevention and recovery campaigns remains “primarily Caucasian men aged 25-35.” Kenyon said data from 2016 to 2018 indicates that 10% of accidental overdose fatality victims were Latinx, and 7% were Black.
In 2019, men accounted for 73% of overdose deaths statewide. The age group with the highest overdose death toll that year (27%) was individuals aged 35-44, while adults who were 25-34 comprised 25%. More than 40% of overdose fatalities were older than 45.
Kenyon said that as of June 2018, when Providence Safe Stations recorded 100 individuals who had entered the station to seek help, “the average [age] was 41, but with a range from 23 to 67.”
The same diversity exists socioeconomically, according to EMTs.
“When I was new to the job, I was kind of surprised because I didn’t really know it was so widespread, but then you see enough of it that you’re not as thrown by seeing it in different environments,” said Farley, “I’ve given Narcan to somebody that’s wearing rags, sitting on the sidewalk somewhere, and I’ve taken an overdose call at a million dollar house. It’s truly across the board.”
Given naloxone’s almost negligible side effects, Rhodes urges both civilians and medical personnel to learn the signs of an overdose and give Narcan a try if they suspect that one might be happening.
“I can recall one case in the state where there were some folks in a car on a highway,” said Rhodes. “Three or four of them had overdosed. They thought they were using cocaine and it was laced with fentanyl.”
Seeing their unconscious bodies and no needle, medical personnel couldn’t immediately confirm that there were opioids involved, but they quickly spotted the other telltale signs.
“EMS was astute enough to go ahead and give naloxone anyway,” Rhodes said, “and it kept those folks alive.”
— Hal Triedman and Iris Lee did the data processing and analysis for this story; graphics by Jane Yue Yang